The virus in an app
My Twitter timeline has featured requests to engage with the COVID symptom tracker website and application (https://covid.joinzoe.com/). I have and I want to make a comment or two about how it’s phrased and what it, well, might mean.
My main issue with the application is that right from the beginning it asks people to rate their symptoms. Here is the screenshot of the first page of the application:

And here we come to the first and significant issue I have with the application. The issue is that we, patients, don’t have symptoms. Basically, as a patient, I only have some (unpleasant) experiences, which the will (or will not) take into account when giving me the diagnosis. By virtue of the doctor’s knowledge and experience and, indeed, the diagnostic criteria, those unpleasant experiences will be turned into medical symptoms which, in the process, will be treated by the doctor. If you need some more on symptoms, please read a recent paper by Kirsti Malterud and her colleagues.
You could, of course, argue that ‘we all’ know exactly what the doctor (or the application) asks you about and I am just splitting hairs. Well, I might be. But before I respond, let me show you another screen shot. This time the application asks for considerably more than simply a ‘description’ of symptoms. This time, the app user is asked to make further assessment:

The app user is asked to make an assessment of significance of their symptoms. Yes, the application explains (sort of) how to make such an assessment, and yet, things are a bit more complicated. First of all, the options are quite ambivalent. It might be me, but I struggle to identify ‘ordinary activity’. Does it mean sitting at my desk and writing a blog, or does it mean hard hoovering? Surely, the two activities imply a different level of exertion and you can only wonder which one is meant by the authors of the application. Similarly, I think that the phrase ‘at rest’ is also somewhat problematic. Do you mean when I have been lying down for half an hour and just sat down on a chair? But that’s not all. Such ambivalence is also introduced elsewhere. What are ‘unusual’ pains? Will I simply know when I have them?
The spectrum of mild – significant – severe (quite commonly found in medicine) is not only about the intensity of symptoms. I am having trouble with the word ‘significant’ which can mean ‘worthy of attention’ and ‘indicative of something’. What kind of judgement are you asking me for? Of course, you could argue again that we, regular patients, can simply make a judgement about the spectrum of little, a bit more, and a hell of a lot, but is this what we’re asked for? The word ‘significant’ introduces ambivalence which makes it all that harder to make the judgement. And this raises the question of whether app users, like me, make similar judgements when we press the options, and, if not, does it matter? It’s worth mentioning that there is significant research about patients lying about their ‘symptoms’, for example, because they don’t want to make a fuss (Kristian Pollock’s research comes to mind). Is it possible that such things happen here?
In the case of shortness of breath, the application does contain explanation. When it asks about fatigue, people’s judgement is unsupported:

Note that the scale is different – from mild to severe, there no significant fatigue (why?). I also find it hard to believe that the experience of fatigue people can have is one between nebulous ‘mild’ and not being able to get out of bed. Incidentally, when you live on your own, you have no bloody choice, do you?
Interestingly, the application introduces yet another judgement:
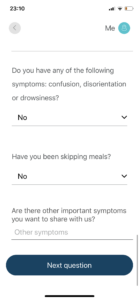
Here it asks me to make a judgement about ‘important’ symptoms. Bloody hell, that’s a bit much, isn’t it? How do I decide whether the symptoms are important (as opposed to significant)? Yes, again, you could argue that it’s for the researchers to make such a judgement. Except before they do, I still need to write it.
I also find it extraordinary that three questions can be answered with one answer. Do note that the question: “Do you have…confusion, disorientation, drowsiness?” are three questions. and yet, only one answer is necessary to answer. That’s badly done, I think.
So, why is it important? Why do I moan again instead of congratulating the researchers at King’s College? After all, at the very least, they’re doing something and I, the grand spoilsport, am moaning about it.
Well, there are a couple of answers. First, in my view, it’s very important to preserve people’s right to a story, even the one reduced to an application choice. I am tired of being asked about my symptoms, and even more tired of bewildered looks on doctors’ faces when I tell them that I don’t have symptoms. ‘When, on a number of occasions, I said symptoms were the doctor’s job, I was looked at with incredulity. I still remember a young doctor looking at me very suspiciously when I mentioned diagnostic criteria of hypertension. It was like I was stealing something from them. We’ should stop this incessant medicalisation of people’s experiences and of clinical interactions.
There is a large body of research on representing experience in medical terms. Indeed, there is also quite a lot of critical research that shows patients taking on medical or semi-medical language when speaking to doctors. It goes even further – as Konrad Opalinski and I showed, insight into schizophrenia was understood by psychiatrists as medical knowledge. They wanted their patients to read up on psychiatry! More and more, illnesses are described only in terms of symptoms. In order to look ‘intelligent’ I must follow suit. Do I still have the right to my own story?
The moment I think about symptoms, at least to an extent I forget about my life. And illness, as has been said a zillion times, is social, while the doctor should treat me, Dariusz Galasinski, a professor, a dad, and an ice-cream lover and certainly not only my symptoms! The moment I start speaking about symptoms I lose all that. I lose the ability to tell me illness story. And that’s the somewhat pernicious side of it.
So, does it all mean that the application is not worth doing? No, of course it doesn’t. I’m sure the brave researchers at King’s will have their crafty ways to reduce what they get even further into wonderfully computable chunks of information. And it will probably be useful. And yet, I still think that ‘we’ shouldn’t undermine the patient’s ability to tell a story.
On final point I want to make about the app is the nifty sleight of hand through the use of the word ‘description’. The word suggests a certain objectivity, the ability to simply access the symptoms and report. It’s worth pointing out that this utter nonsense. Just as we construct an illness in our stories, we do in the app provided. The application does not give anyone objective data to look it. It gives those reduced-to-nothing stories which must be fitted into an application. Like it or not, the world of the coronavirus is now an app.